Cytek Investor Day Presentation Deck
Multicolor Flow Combined With Next Gen Sequencing
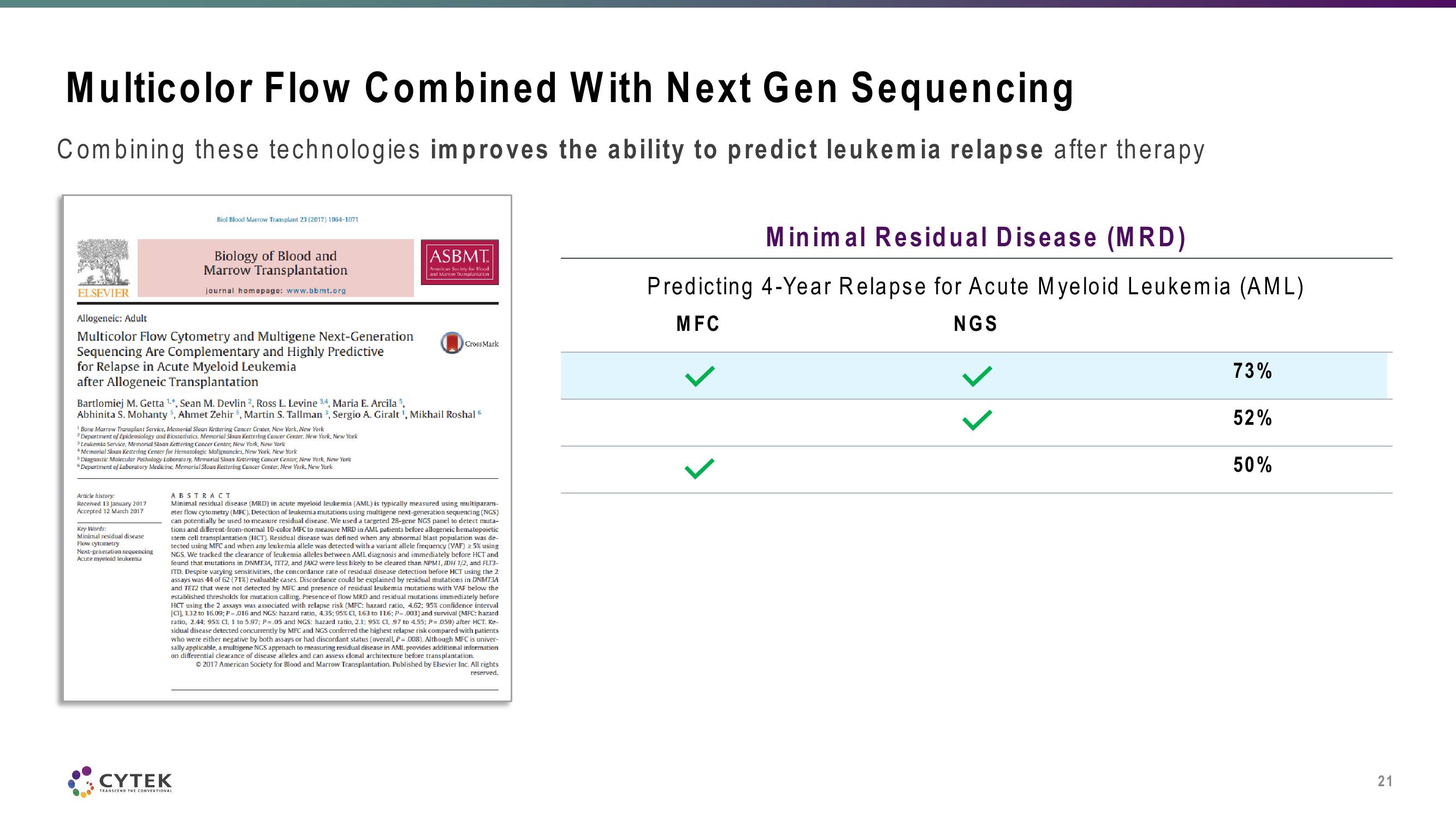
Combining these technologies improves the ability to predict leukemia relapse after therapy
ELSEVIER
Allogeneic: Adult
Multicolor Flow Cytometry and Multigene Next-Generation
Sequencing Are Complementary and Highly Predictive
for Relapse in Acute Myeloid Leukemia
after Allogeneic Transplantation
Biol Blood Marrow Transplant 23 (2017) 1064-1071
¹ Bone Marrow Transplant Service, Memorial Sloan Kettering Cancer Center, New York, New York
2 Department of Epidemiology and Biostatistics, Memorial Sloan Kettering Cancer Center, New York, New York
* Leukemia Service, Memorial Sloan Kettering Cancer Center, New York, New York
4 Memorial Sloan Kettering Center for Hematologic Malignancies, New York, New York
Article history:
Received 13 January 2017
Accepted 12 March 2017
Biology of Blood and
Marrow Transplantation
journal homepage: www.bbmt.org
Bartlomiej M. Getta ¹.*, Sean M. Devlin 2, Ross L. Levine 3,4, Maria E. Arcila 5,
Abhinita S. Mohanty 5, Ahmet Zehir 5, Martin S. Tallman ³, Sergio A. Giralt ¹, Mikhail Roshal 6
Diagnostic Molecular Pathology Laboratory, Memorial Sloan Kettering Cancer Center, New York, New York
* Department of Laboratory Medicine, Memorial Sloan Kettering Cancer Center, New York, New York
Key Words:
Minimal residual disease
Flow cytometry
Next-generation sequencing
Acute myeloid leukemia
CYTEK
TRANSCEND THE CONVENTIONAL
ASBMT
American Society for Blood
and Marrow Transplantation
Cross Mark
ABSTRACT
Minimal residual disease (MRD) in acute myeloid leukemia (AML) is typically measured using multiparam-
eter flow cytometry (MFC). Detection of leukemia mutations using multigene next-generation sequencing (NGS)
can potentially be used to measure residual disease. We used a targeted 28-gene NGS panel to detect muta-
tions and different-from-normal 10-color MFC to measure MRD in AML patients before allogeneic hematopoietic
stem cell transplantation (HCT). Residual disease was defined when any abnormal blast population was de-
tected using MFC and when any leukemia allelle was detected with a variant allele frequency (VAF) 25% using
NGS. We tracked the clearance of leukemia alleles between AML diagnosis and immediately before HCT and
found that mutations in DNMT3A, TET2, and JAK2 were less likely to be cleared than NPM1, JDH 1/2, and FL13-
ITD. Despite varying sensitivities, the concordance rate of residual disease detection before HCT using the 2
assays was 44 of 62 (71%) evaluable cases. Discordance could be explained by residual mutations in DNMT3A
and TET2 that were not detected by MFC and presence of residual leukemia mutations with VAF below the
established thresholds for mutation calling. Presence of flow MRD and residual mutations immediately before
HOR
HCT using the 2 assays was associated with relapse risk (MFC: hazard ratio, 4.62; 95% confidence interval
[CI], 1.32 to 16.09; P=.016 and NCS: hazard ratio, 4.35; 95% CI, 1.63 to 11.6; P=.003) and survival (MFC: hazard
ratio, 2.44; 95% CI, 1 to 5.97; P=.05 and NGS: hazard ratio, 2.1; 95% CI, 97 to 4.55; P=.059) after HCT. Re-
sidual disease detected concurrently by MFC and NGS conferred the highest relapse risk compared with patients
who
were either negative by both assays or had discordant status (overall, P = .008). Although MFC is univer-
sally applicable, a multigene NGS approach to measuring residual disease in AML provides additional information
on differential clearance of disease alleles and can assess clonal architecture before transplantation.
©2017 American Society for Blood and Marrow Transplantation. Published by Elsevier Inc. All rights
reserved.
Minimal Residual Disease (MRD)
Predicting 4-Year Relapse for Acute Myeloid Leukemia (AML)
MFC
NGS
73%
52%
50%
21View entire presentation